OC Guidance on Safeguarding g, Mental Capacity, Deprivation of Liberties and the Prevent Strategy
Protecting Children and Adults at risk
Updated August 2019
Summary
Abuse, neglect, female genital mutilation (FGM), coercive behaviour, trafficking and radicalisation are often hidden in our society but can reveal themselves in a health care situation including during occasional health interactions.
This is why safeguarding children and adults at risk is an overriding professional duty for all registered optical practitioners and practices in the same way as for other health and social care practitioners and providers.
Part 1 of this guidance provides a simple five step guide for all optical staff and practices to safeguard children and adults at risk and to comply with all relevant legislation. It will help you to be vigilant, able to recognise and report abuse, and help keep your patients and colleagues safe. This part of the guidance has been updated in August 2019 in line with the revised Intercollegiate Guidance for Safeguarding Children (2019) and Intercollegiate Adult Safeguarding for Health Care Staff (2018).
Part 2 of this guidance sets out the responsibilities of optical staff and practices under the UK-wide Prevent Strategy. This requires healthcare providers to work with partner organisations to identify individuals at risk of radicalisation and to refer them to regional Prevent teams for support. The steps to follow in such cases are similar to those for safeguarding other adults, young people and children who are at risk.
ACTION
Practices should ensure that all staff1 are familiar with this guidance and know what to do if they suspect or observe signs or symptoms of suspected abuse, neglect, FGM, coercive behaviour, trafficking or radicalisation.
A copy of this guidance including
- up-to-date local Safeguarding team contact information
- up-to-date Prevent team contact information
should be readily available in all practices.
1 All staff means all staff including receptionists and back office staff and not just registrants or staff in patient facing roles. Anyone can spot patterns or unusual behaviours in any role at any time.
NHS England and/or Local Health Boards should regularly notify practices of up-to-date contact information for local Safeguarding and Prevent teams.
If, for some reason, this is not available, up-to-date safeguarding information can be found via the link below or by downloading the apps
www.myguideapps.com/nhs_safeguarding/default/
play.google.com/store/apps/details?id=com.antbits.nhsSafeguardingGuide&hl=en_GB
itunes.apple.com/gb/app/nhs-safeguarding-guide/id1112091419?mt=8
Prevent team contact information should be available on the local police or Council website but local arrangements can vary. In practice it is probably best to search the Internet for ‘Contact my local Prevent team’.
Registered practitioners should ensure that they understand their professional duties under this guidance and have completed appropriate training to Intercollegiate Level 2 for safeguarding children and adults at risk.
Pre-registration practitioners and students on placements should have the same understanding as registered practitioners by, as a minimum, having read and understood this guidance.
In the case of registered practitioners in Scotland this means also holding a current Protection of Vulnerable Groups (PVG) certificate for each health board where you practise. If you are applying to join a health board’s ophthalmic list your PVG certificate must be dated within 28 days of application.
This guidance will continue to be updated periodically as legislation is revised and in the light of experience.
Remember: if you feel uncomfortable about a particular situation, have concerns about a patient’s or other person’s safety and suspect abuse or radicalisation, you must record the facts and raise the issue with an appropriate person or organisation. This may be a designated or senior person in your organisation, your professional or representative body, or a local safeguarding official.
Part 1: Safeguarding children and adults at risk
What to do if you observe/suspect abuse or neglect
Any optical practitioner or member of practice staff who detects possible signs of neglect or abuse in a child or adult (including possible domestic or elder abuse) should take immediate action as below.
1. Observe
Note factual signs and symptoms of potential or suspected abuse or neglect without alarming the child or adult concerned or alerting a possible abuser.
If appropriate, listen sympathetically to what a child or adult tells you (as they are often ignored) but do not agree not to tell anyone what they have told you.
2. Discuss
Do not delay. Discuss your concerns with your manager, senior professional, designated staff member or, if you are a pre-registration optometrists with your supervisor, depending on your practice procedure.
If appropriate, seek advice from the local authority safeguarding team.
Remember, particularly in the case of a child, you may be the only person to have noticed anything unusual or whom they have confided in. You therefore have a professional duty to act as their advocate. This means making sure that the issue is raised with an appropriate person. This is an integral part of being a healthcare professional in a privileged position of authority and trust.
Information Sharing
If you plan to raise the issue with a safeguarding team or official, you should consider and agree with the person you have discussed the issue with, whether it is appropriate to seek the child’s/ parent’s/person’s agreement to reporting the information, for them to be informed of the report, or whether doing so would place them at increased risk. Seeking the child’s/parent’s/person’s agreement might be appropriate, say, when abuse or radicalisation by a third party, such as an estranged parent, sibling or other person is suspected.
Relevant personal information can be shared lawfully if it is to keep a child or individual at risk safe from neglect or physical, emotional or mental harm, or if it is protecting their physical, mental, or emotional well-being. The Data Protection Act 2018 specifically includes ‘safeguarding of children and individuals at risk’ as a condition that allows practitioners to share information without consent. Information can be shared legally without consent, if a practitioner is unable to, or cannot be reasonably expected to, gain consent from the individual, or if seeking consent could place a child or adult at risk.
3. Act
If appropriate, inform your local safeguarding team and supply them with a copy of your recorded observations (using the model referral form at Annex 3).
When reporting information, reports should be restricted to
- the nature of the injury, suspicious behaviour or concern
- facts which support the
You and the person with whom you are sharing the information must agree what the patient/relatives/legal guardians/carers/person will be told, by whom and when, and you should keep a note of what has been agreed together with a copy of the referral form.
4. Confirm
Confirm telephone notifications in writing by fax, email or letter within 48 hours. If you are using a non-secure method of communication consider anonymising or password protecting the notification.
You should receive confirmation of referral within one working day. If you have not heard back within three working days, contact again. Keep contacting (including considering using another route) until you receive confirmation of receipt or other substantive communication or advice.
If you are/will not be available to do this, make sure by agreement with an appropriately senior person in the practice that this will happen and record that agreement as part of Step 5 below.
5. Record
Ensure that all observations, advice sought, advice received and actions taken are recorded and stored confidentially and separately from the patient’s optical record.
In the unlikely event that you come across an individual in optical practice who is at immediate risk of harm, contact the police.
Be Vigilant
Awareness is by far the greatest protection for children and people at risk. See Annex 1
- what to look out for – common signs and symptoms of abuse or neglect
- what to look out for – inappropriate staff behaviour towards a patient
Any optical practitioner or member of staff who detects inappropriate behaviour by a colleague (also described in Annex 1) should take immediate action by following the five steps outlined above.
Local Advice and Support for Safeguarding
All local authorities in England, Wales, Scotland and Northern Ireland have duties to make arrangements to promote co-operation and co-ordination between local agencies regarding local protection procedures, including NHS England Regional Teams and Local Health Boards (LHBs).
In England and Wales local authorities have duties under the Children Act 2004 to promote cooperation between themselves, NHS England Regional Teams and Local Health Boards to improve the wellbeing of children, to make arrangements when carrying out their normal functions to safeguard and promote the welfare of children, and to establish a Local Safeguarding Children Board (LSCB).
Across the UK specialist safeguarding experts are available to provide advice and support to local practices and practitioners about whether to make a referral of suspected abuse or neglect.
In the case of children in England, Wales and Northern Ireland designated safeguarding doctors or nurses and protection officers perform these functions.
In England, every Clinical Commissioning Group (CCG) is required to have a designated safeguarding doctor and designated safeguarding nurse.
Public Health Wales has a structure of designated and named safeguarding professionals in each of the seven health boards.
In Northern Ireland, each Health and Social Services Trust has designated professionals for child protection.
In Scotland child protection advisors and nurse consultants fulfil this role. Some health boards in Scotland also have Child Protection Nurse Advisors.
All NHS England Regional Teams and CCGs should issue health care providers, including all optical practices, with up-to-date
- local guidance if appropriate
- local safeguarding team contacts for advice or referral
- information on local training opportunities
- details of the designated doctor and nurse available for advice and The contacts for relevant local safeguarding teams/officials should be
- able to receive confidential information 24 hours a day
- prepared to give advice to front-line optical staff and practices in respect of safeguarding children and adults at risk
(NB the local contacts are likely to be different for children and adults at risk.)
Optical practice managers should ensure these contact details are readily available in the practice. If you have any problem identifying the correct person in your area, please contact your LOC/ROC/AOC or local NHS professional or management contacts.
Safeguarding Training for Optometrists and Opticians
All optometrists, contact lens and dispensing opticians should complete safeguarding training to Level 2 of the Intercollegiate Safeguarding Guidance for Adults (2018) and children (2019). They should then receive refresher training equivalent to a minimum of 3-4 hours at least every three years.
Practices should incorporate these requirements into CET planning and annual appraisal systems.
Safeguarding Training for Other Practice Staff
All non-registered practice staff should complete safeguarding training to Level 1 of the Intercollegiate Safeguarding Guidance for Adults (2018) and children (2019).
This can be achieved by all non-registered staff studying this guidance, discussing anything they do not understand or any concerns they have with their manager, senior professional or designated staff member (see page 2, section 2) and signing to acknowledge they have read and understood the contents and know what steps to take should a situation arise with regard to safeguarding or Prevent. A template form for this is at Annex 6. Practices should file and retain staff forms for reference purposes. Refresher training should be undertaken every three years.
Studying this guidance and discussing any points that are unclear with a manager is sufficient to meet level 1 requirements of the Intercollegiate Guidance for Adults (2018) and children (2019).
Female Genital Mutilation
If you have any concerns regarding FGM in respect of a patient or any other person under 18 you should follow the steps in this guidance.
All healthcare professionals in England and Wales have a legal obligation to report any case of FGM in girls under the age of 18 to the police by telephoning 101 or 999 if there is an immediate risk.
If there is no immediate risk, you can also contact the National Society for the Prevention of Cruelty to Children on 0800 028 3550.
Further guidance on FGM is available from the Department of Health and Social Care.
Participation in Safeguarding Assessments/Plans
People who have been victims, or who are at risk, of abuse or neglect have the same eye health needs and health care rights as other members of society.
Social services may ask optical practices and practitioners to provide information about patients they have examined, or to take part in safeguarding assessments. They may also ask practitioners to provide eye care services to patients as part of a locally agreed safeguarding plan for those individuals.
If the practice or practitioner chooses to provide these eye care services local protocols and guidelines should be followed.
GP or Hospital Referrals
Optical practitioners may need to refer patients with suspected abuse or neglect to their GP or hospital e.g. if the practitioner notices a retinal haemorrhage. In such cases, practitioners should continue to refer the ocular/general health issue as normal, and in parallel, follow the five steps above, making the GP or hospital referral known to the local safeguarding team.
Mental Capacity and Deprivation of Liberty Safeguards
People who lack the mental capacity to make certain decisions for themselves, for example with regard to their medical care or entering into sales contracts, are considered particularly at risk. Lack of capacity is usually the result of a disability, mental or physical condition or trauma that affects the way the mind or brain works. This can be a temporary or permanent condition and can affect a broad range of decisions or only decisions on a certain issue.
Mental Capacity and Deprivation of Liberty Safeguards were introduced as part of the Mental Capacity Act 2005 to give protection to people who lack mental capacity.
The Mental Capacity Act sets out five statutory principles to protect people who lack capacity to make particular decisions, but also to maximise their ability to make decisions, or to participate in decision-making, as far as they are able. Professionals working with people who may lack capacity should be guided by these principles and the supporting examples set out in the Act.
The five statutory principles are:
- A person must be assumed to have capacity unless it is established that they lack
- A person is not to be treated as unable to make a decision unless all practicable steps to help them to do so have been taken without success.
- A person is not to be treated as unable to make a decision merely because they make an unwise decision.
- An act done, or decision made, on behalf of a person who lacks capacity must be done, or made, in their best interests.
- Before the act is done, or the decision is made, consider whether the outcome can be achieved as effectively in a way that is less restrictive of the person’s rights and freedom of
NHS Standard Contract holders in England are required to nominate a Mental Capacity and Deprivation of Liberty Lead. This person would be expected to have a working knowledge of the relevant legislation and be in a position to provide support and advice.
Very occasionally in the case of eye care, Deprivation of Liberty Safeguards (DoLS) can be used to compel a person who lacks capacity to accept medical treatment. In such cases there are strict legal standards to ensure that any action taken is in the person’s best interests and that the intervention is minimally restrictive.
Part 2: Playing your part in the Prevent Strategy
The Prevent Strategy is part of the UK-wide counter-terrorism strategy to which the NHS is a signatory. The Prevent agenda requires healthcare organisations to work with the police to contribute to the prevention of terrorism.
The definition of ‘at risk’ has been widened to include individuals who might be at risk of being radicalised. These individuals should be identified and referred to the regional Prevent team contacts for appropriate advice and support. Advice on signs that an adult or child may have been or is being drawn into terrorism are at Annex 2.
Practices should ensure that they have procedures in place to allow for the referral of such individuals to local Prevent team contacts.
Prevent team contact information should be available on the local police or Council website but local arrangements can vary. In practice it is probably best to search the Internet for ‘Contact my local Prevent team’.
As in other safeguarding situations, the following steps should be followed:
1. Observe
Note factual signs and symptoms of potential or suspected radicalisation without alarming the person or colleague concerned.
2. Discuss
Alert and discuss your concerns with your manager, senior professional, designated staff member or, if you are a pre-registration optometrists with your supervisor, depending on your practice procedure.
If appropriate, seek advice from the local NHS Prevent team.
3. Act
If appropriate, inform the local NHS Prevent team and supply them with a copy of your recorded observations (using the model referral form supplied in Annex 4).
When reporting information, reports should be restricted to
- the nature of the suspicious behaviour or concern
- facts which support the
4. Confirm
Confirm telephone notifications in writing by email, secure fax or letter within 48 hours. If you are using a non-secure method of communication, consider anonymising or pass word protecting this notification.
You should receive confirmation of referral within one working day. If you have not heard back within three working days, contact again. Keep contacting (including considering using another route) until you receive confirmation of receipt or other substantive communication or advice.
If you are/will not be available to do this, make sure by agreement with an appropriately senior person in the practice that this will happen and record that agreement as part of Step 5 below.
5. Record
Ensure that all observations, advice sought, received and actions taken are recorded and stored
confidentially and separately from the patient’s optical record.
Given the nature of optical practice and frequency of contact with patients, cases of suspected radicalisation amongst patients should be rare. However colleagues or other acquaintances may show these signs. If you have any concerns or questions, please contact your Optical Confederation representative body for advice and assistance.
Part 3: Responsibilities of for Optical Practitioners, Staff and Practices
Practice Protocol
Each optical practice should
- have safeguarding and Prevent protocol/procedures in place in line with this guidance and guidance from the College of Optometrists
- ensure that all members of staff and practitioners are aware of and understand the protocol/procedures.
Safeguarding and chaperone policies should already be in place as part of GOS compliance. However it is worth noting that the protocol/procedures should include:
- the appointment of the practice manager or another nominated senior professional as the responsible person within the practice to whom members of staff should refer safeguarding and Prevent concerns in the first instance
- a chaperone policy – a sample policy can be found at qualityinoptometry.co.uk
- a copy of this guidance in the practice
- local safeguarding team contact details
- local NHS Prevent team contact details
- a copy of any relevant local safeguarding guidance
- the procedures staff should follow where the nominated responsible person is unavailable (or inappropriate) g. contact number at company headquarters or a direct contact number to local safeguarding or NHS Prevent team.
Practitioners and Staff
- Be familiar with the common signs and symptoms of abuse, neglect or radicalisation and the
meaning of the term ‘looked after child’ (Annexes 1 and 2).
- Understand that for safeguarding purposes, a child or young person is defined as someone who has not yet reached their 18th birthday
- Be alert to any signs of more widespread abuse g. in siblings or others attending with the patient
- Take personal responsibility for referring cases of suspected abuse, neglect or radicalisation of a patient by a family member, carer, or any other person, including for domiciliary patients a care home staff member, to the responsible person in the practice or other appropriate person
- Take personal responsibility for referring suspected abuse or neglect by an optical practitioner or a member of practice staff to an appropriate Staff should speak to the responsible person in the practice.
- The responsible person in the practice should apply their professional judgement to each case and should not make assumptions about a case on the basis of familiarity or assumed knowledge of the situation. Stick to observed facts and, if in any doubt, refer to the safeguarding or Prevent specialists.
Practices
- Fixed practices should identify a lead clinician in the practice with responsibility for safeguarding and Prevent procedures and ensure all staff are aware of who this is
- Domiciliary and mobile providers should similarly nominate a lead clinician and make all staff aware of who this is
- All practices should respond helpfully to a formal request by social services to provide information about a patient who is involved in a safeguarding assessment or to provide eye health services to a child or adult at risk as part of an agreed safeguarding plan
- All practices should play their part in identifying individuals at risk of being radicalised or involved in terrorist related activities, and refer them for further support.
Further Information
Details of relevant legislation and guidance are at Annex 5. For further information please contact your representative body or professional association.
ABDO members Katie Docker kdocker@abdo.org.uk
AOP members Regulatory Team regulation@aop.org.uk
FODO members Member Support Team info@fodo.com
Optical Confederation
Originally published: 2014, updated 2017, updated August 2019
What to look out for – common signs and symptoms of abuse or neglect
Reminder: The Optical Confederation advises that all staff should speak to the practice’s lead clinician if they see any signs or symptoms of abuse or neglect, who should in turn seek professional advice from the local designated doctor or nurse. Your representative body is also available to advise on specific cases.
Children
Physical abuse
Eye injuries, unexplained retinal haemorrhage, fractures, hypothermia, lacerations, subdural haemorrhage, teeth marks, scalds, scars, petechiae (small haemorrhages on the skin), abrasions, bites, bruises, burns, cold injuries (e.g. swollen, red hands or feet), cuts, bites, wearing inappropriate clothes e.g. long sleeves even in hot weather; fear of physical contact – shrinking back if touched – bald patches, aggression.
Neglect
Bites, dirty clothing, dirty child, head lice, persistent infestations, scabies, sunburn, tooth decay, not complying with treatment / advice.
Emotional/behavioural abuse
Age-inappropriate behaviour, aggression, body-rocking, changes in emotional or behavioural state, fearfulness, runaway behaviour, continual self-deprecation (I’m stupid, ugly, worthless, etc), overreaction to mistakes, extreme fear in new situations, neurotic behaviour (rocking, hair-twisting) extremes of passivity or aggression.
Sexual abuse
Sexualised behaviour, age-inappropriate behaviour, regressive behaviour, being overly affectionate, being isolated and withdrawn, inability to concentrate, lack of trust or fear of someone they know well.
Parents and children
Be alert to any signs of more widespread abuse, e.g. in siblings or others attending with an adult patient.
Other
Abuse might manifest in other ways, for example mental ill-health, alcohol or drug misuse.
You should also be generally aware of the potential for the internet or social media to be used to perpetrate abuse.
Trafficking and female genital mutilation (FGM)
Child trafficking and female genital mutilation (FGM) are forms of abuse and should be addressed in exactly the same was as any other form of abuse.
Looked After Children
This term is used to describe any child who is in the care of the local authority or who is provided with accommodation by the local authority social services department for a continuous period of more than 24 hours. This covers children in respect of whom a compulsory care order or other court order has been made. It also refers to children accommodated voluntarily, including under an agreed series of short-term placements which may be called short breaks, family link placements or respite care.
Adults
Physical abuse
Unexplained falls or major injuries, injuries/bruises at different stages of healing, bruising in unusual sites e.g. inner arms, abrasions, teeth indentations, injuries to head or face, very passive.
Elder abuse
As above, plus hand-slap marks, pinches or grip marks, physical pain, burns, blisters, unexplained or sudden weight loss, recoiling from physical contact, stress or anxiety in presence of certain individuals, perpetrator describing person as uncooperative/ungrateful/unwilling to care for self, restraint, unreasonable confinement e.g. locking in or tying up.
Psychological abuse
Withdrawal, depression, cowering, fearfulness, agitation, confusion, changes in behaviour, obsequious willingness to please, no self-esteem, fear, anger.
Domestic abuse
Bruises, black eyes, painful limbs, make-up covering bruises, damaged clothes or accessories, patient “walking on eggshells” if partner around, partner belittling or putting down patient, partner acting excessively jealously or possessively, partner insisting on accompanying patient at all times, partner nervous if patient is out of their sight, patient having limited access to money, phone, car etc.
Other
Abuse might also manifest as mental ill-health, alcohol or drug misuse. Non Verbal Communication / Indirect Signalling
Be alert for indirect forms of signalling or silent cries for help. For instance some abused children, young people or adults may be unable to articulate or speak about what may be happening to them but may try to communicate with the practitioner in other ways e.g. rolled-up sleeves, low necks or shorts which reveal bruises or injury sites.
Colleagues and Staff Warning Signs
Colleagues or staff paying particular attention to a patient or a group of patients (e.g. young children, girls, boys), appearing overfriendly with particular patients, families or groups, going out of their way
to see the same patient without obvious reason, seeming overly familiar with a patient, always seeking out a particular patient or changing a patient’s appointments to fit in with times when they are present without clinical reason, patient request or established professional relationship.
Prevent Strategy: Signs that a Person is Being Radicalised
A member of the practice team may have concerns relating to an individual’s behaviour, which could indicate that they may be being drawn into terrorist activity. This might include other members of the practice team.
Radicalisation can be difficult to spot. Signs or indicators that someone is being drawn into terrorist activity may include:
- Graffiti symbols, writing or artwork promoting extremist messages or images
- Patients/staff accessing terrorist related material online, including through social network sites
- Parental/family reports of changes in behaviour, friendships or actions, coupled with requests for assistance
- Partner healthcare organisations’, local authority services’ and police reports of issues
affecting patients in other healthcare organisations
- Patients voicing opinions drawn from terrorist related ideologies and narratives
- Use of extremist or hate terms to exclude others or incite Signs that may indicate a child is being radicalised include:
- isolating themselves from family and friends
- talking as if from a scripted speech
- unwillingness or inability to discuss their views
- a sudden disrespectful attitude towards others
- increased levels of anger
- increased secretiveness, especially around Internet
Individuals who are at risk of radicalisation may have low self-esteem, or be victims of bullying or discrimination. Extremists may target them and tell them they can be part of something special, later brainwashing them into cutting themselves off from their friends and family.
In the case of children, these signs do not necessarily mean a child is being radicalised – it may be normal teenage behaviour or a sign that something else is wrong.
Nevertheless, if you notice any of these signs or indicators, you should follow the five step protocol set out in Part 2 of this guidance.
In the case of children, the National Society for the Prevention of Cruelty to Children (NSPCC) helpline on 0808 800 5000 can also offer advice.
CONFIDENTIAL
NOTIFICATION OF POTENTIAL CHILD OR ADULT ABUSE OR NEGLECT
To be completed by the referring practitioner
This form notifies the appropriate person at the Regional Team/Health Board and/or at the Child Safeguarding Team of suspected abuse.
SUSPECTED VICTIM
Name: Address:
Gender:
Date of Birth:
Name of Person with parental responsibility/Carer/Next of Kin
Relationship Other identifiers:
SUSPECTED PERPETRATOR (if known)
Name: Address:
Age if under 18: Relationship if known: Other:
FORM OF SUSPECTED ABUSE OR NEGLECT
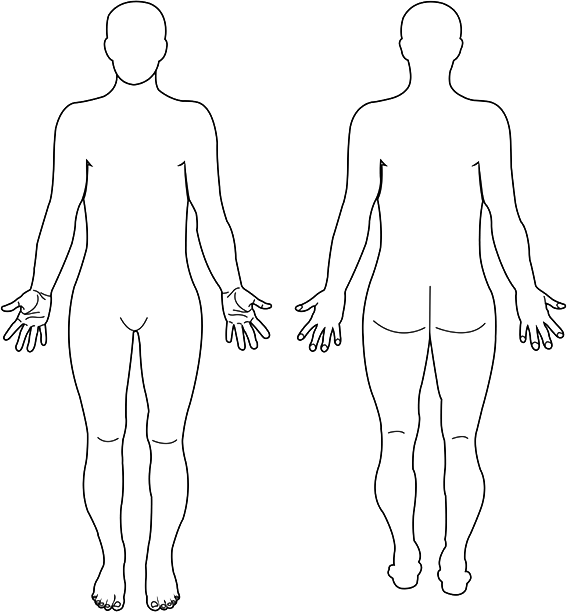
(Include body map – Annex 7 – to indicate body positions or marks where relevant.)
WHETHER SUSPECTED VICTIM/PARENT/CARER AGREED TO OR HAS BEEN INFORMED OF THE REFERRAL
Yes/No
DISCLOSURE AGREEMENT (with Recipient of Referral about what patient and suspected perpetrators will be told, by whom and when)
Declaration:
I wish to make this notification in line with the disclosure agreement above unless
- I have been further approached and have specifically given my permission in writing in advance for the release of my details, or
- the release of my details is ordered by a UK
MEANS OF TRANSMISSION:
Telephone
Secure Fax
Secure email
Registered Letter
This is a first referral/follow-up confirmation Signature……………………………………………………………
Print Name………………………………………………………….
Position………………………………………………………………
Date…………………………………………………………………….
Download editable form here Annex 3 Safeguarding
CONFIDENTIAL
NOTIFICATION OF POTENTIAL PREVENT CONCERN
To be completed by the referring practitioner
This form notifies the appropriate person at … Health Board and/or at … Local Authority of suspected Prevent concern.
SUSPECTED INDIVIDUAL BEING RADICALISED
Name: Address:
Gender:
Date of Birth:
Name of Person with parental responsibility/Carer/Next of Kin (if appropriate)
NATURE OF SUSPICION (detail of concerns/observations)
MEANS OF TRANSMISSION:
Telephone
Secure Fax
Secure email
Registered Letter
This is a first referral/follow-up confirmation Signature……………………………………………………….
Print Name…………………………………………………….
Position…………………………………………………………
Date………………………………………………………………
Download editable form here Annex 4 Safeguarding
<strong>Legislation, Regulations, National and Professional Guidance</strong>
<ul>
<li>Children Act 1989 & 2004</li>
<li>Safeguarding Vulnerable Groups Act 2006</li>
<li>Mental Capacity Act (2005): Code of Practice 2007</li>
<li>Children and Young Persons Act 2008</li>
<li>Safeguarding Children in whom illness is fabricated or induced, HM Government 2008</li>
<li>When to suspect child maltreatment, clinical guideline, National Institute for Health and Clinical Excellence, 2009</li>
<li>College of Optometrists guidance: Safeguarding Children: 10 – C1.13, 2010</li>
<li>Building Partnerships, Staying Safe, Department of Health 2011</li>
<li>Protection of Freedoms Bill 2012</li>
<li>Human Trafficking practical guidance, Home Office 2013</li>
<li>The Care Act 2014</li>
<li>Intercollegiate Guidance: Safeguarding Children and Young People: roles and competences for health care staff, 2014</li>
<li>The Right to Choose: Multi-agency statutory guidance for dealing with forced marriage, HM Government 2014</li>
<li>FGM: mandatory reporting in healthcare, Department of Health 2015</li>
<li>Health and Social Care Act 2008, Regulations 2014 & 2015</li>
<li>Statutory guidance on Promoting the Health and Well-being of Looked After Children, Department for Education/ Department of Health 2015</li>
<li>What to do if you’re worried a child is being abused, HM Government 2015</li>
<li>Working Together to Safeguard Children, HM Government 2015</li>
<li>Multi-agency Statutory guidance on Female Genital Mutilation, HM Government 2016</li>
<li>Adult Safeguarding: Roles and Competences for Health Care Staff, Intercollegiate Document 2018</li>
<li>Information sharing – Advice for practitioners providing safeguarding services to children, young people, parents and carers, HM Government 2018</li>
<li>Safeguarding Children and Young People; Roles and Competences for Healthcare Staff, Intercollegiate Document,2019</li>
<li>Safeguarding, Mental Capacity Act and Deprivation of Liberty Primary Eyecare Services Ltd 2019</li>
</ul>
<strong>Registered optical professionals </strong>have a professional duty to make the care of the patient their first and continuing concern. By definition this includes safeguarding them from abuse. (See GOC Standards for Optometrists and Dispensing Opticians and Standards for Optical Students.)
<strong>Registered optical businesses </strong>have a parallel professional duty to ensure that, as a condition of employment or engagement, individual registrants comply with the GOC’s Standards for Optometrists and Dispensing Opticians and Standards for Optical Students. (See GOC Standards for Optical Businesses.)
<strong>Optical providers of NHS services </strong>also have a contractual duty under GOS and, in England under the NHS Standard Contract, to have regard to relevant guidance issued by the NHS or other competent bodies.
<strong>All optical professionals </strong>will need to be aware of how to work with other relevant agencies in accordance with the safeguarding provisions of the Care Act 2014 and must support the work of the Local Safeguarding Children Boards (LSCBs) and Safeguarding Adults Boards (SABs). Optical professionals should understand the key role of LSCBs and SABs in highlighting required improvements with regards safeguarding and act accordingly as necessary.
Optical professionals in England and Wales should be aware of Regulation 13: Safeguarding service users from abuse and improper treatment as one of the fundamental standards of the Health and Social Care Act 2008. They should also be aware of local authorities’ duty to investigate child welfare safeguarding set out in the Children Act 1989.
Optical professionals should be broadly familiar with relevant government guidance about other safeguarding issues. These other issues are female genital mutilation; forced marriage including so-called ‘honour based violence’; fabricated or induced illness; and practical guidance on human trafficking and human slavery. It is recognised that optical clinical examinations will not uncover issues such as FGM; however, optical professionals should still be aware of the issues and the relevant guidance. They should also be aware of adults showing signs of self-neglect including poor personal hygiene, lack of appropriate clothing and failure to meet feeding or medical requirements.
Declaration by non-registered staff member
I confirm that I have read the Optical Confederation’s Guidance on Safeguarding, Mental Capacity, Deprivation of Liberties and the Prevent Strategy, Protecting Children and Adults at risk (Version August 2019).
I have discussed any concerns or points I did not understand with my manager, senior professional, supervisor or designated staff member.
I understand the guidance, my responsibilities and what course of action I should take if I have safeguarding concerns about a child, adult at risk, colleague or individual I believe might be at risk of radicalisation.
Signature:
Name (Print):
Date:
Download editable form here Annex 6 Safeguarding