Dry Eye Corner Part 5
In this month’s Dry Eye Corner, Keith Tempany presents a real-life case study regarding contact lenses and dry eyes. The case will highlight how co-managed care between a community eyecare practice and a hospital ophthalmology department resulted in a life-changing result for the patient.
I make no apology for how this story is written, for it is primarily a human interest story rather than an objective dry eye case study – and it includes excerpts from a letter that the patient, Linda, wrote about her experience.
I would like Linda’s story to inspire eyecare practitioners to look at those challenging contact lens fits with a different perspective, keeping the patient at the heart of your decision making, and being prepared to work with colleagues across the profession. Obviously, names have been changed for anonymity.
Linda’s story
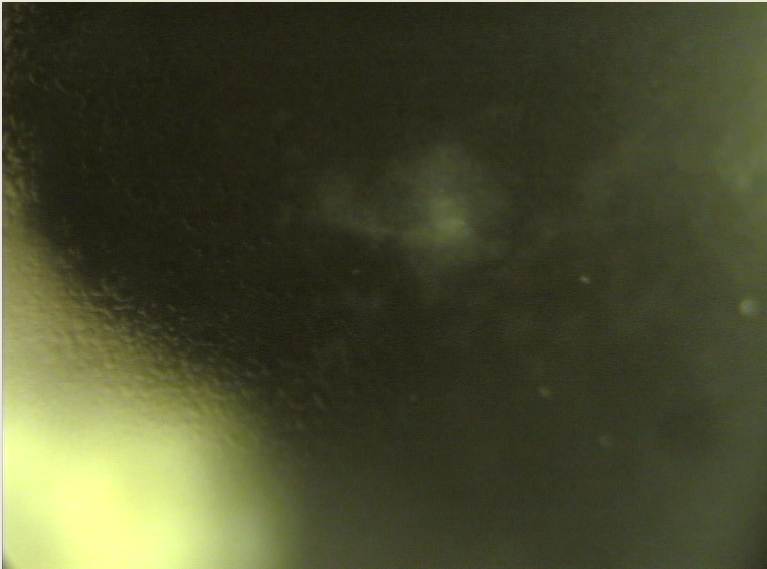
Retro illumination of corneal scarring
I first met Linda – an active, young-at-heart, myopic 74-year-old who had been recommended to see me – regarding her rigid gas permeable (RGP) contact lens. She was only wearing a lens on her right eye.
About six years previously, Linda suffered a shingles attack, which had left her left cornea badly scarred. She was told that she would never be able to wear a contact lens on that eye again.
Her corrected visual acuity was R 6/7.6 L 6/36. The poor vision with the left eye seemed to be due to the corneal scarring, causing an irregular epithelial surface, and punctate keratitis for which she was under ophthalmology for treatment.
Her initial treatment for this eye was steroid drops and lubricants, but currently her dry eye was being managed with viscous lubricating eyedrops four times a day, and eye ointment two to three times a day and overnight. However, her symptoms varied greatly and punctal plugs were suggested by Mr Smith, her ophthalmologist.
“For years, the world dimmed,” wrote Linda. “Both eyes seemed to be affected since they couldn’t seem to work together; my sight seemed off kilter and even my balance was affected. When I looked ahead, half my vision seemed to be opaque.”
Lots of different solutions to her balance issues were apparently tried, including blacking out the left spectacle lens, trying different strength lenses in both contact lens and spectacles.
Her ophthalmologist had recently suggested either tarsorrhaphy (sewing the left eyelids together) or implanting weights in the left upper lid, in order for it to remain closed.
“I couldn’t drive once the light started to fade as the headlight glare caused chaos, because of this I had to give up my Thai Chi, book clubs and knitting group,” Linda wrote. “Luckily, I am a naturally optimistic person, but there were days…”
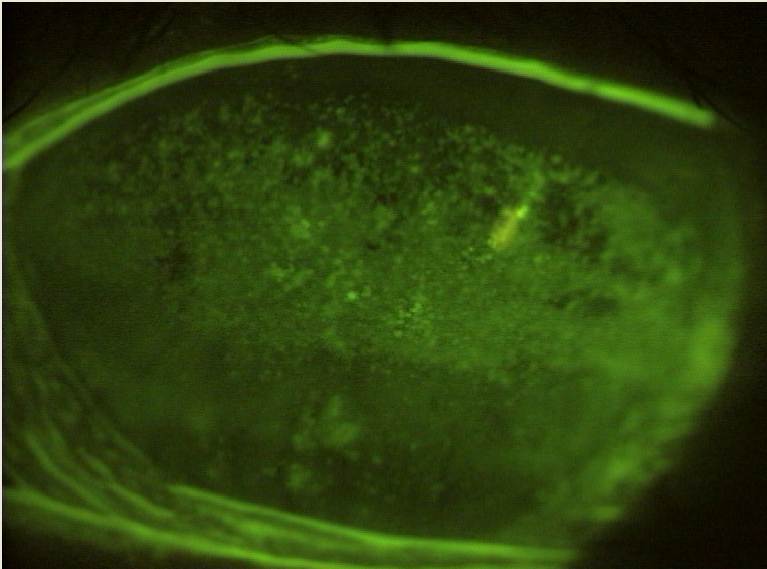
Fluorescein staining of corneal scarring
Linda was not enamoured with either having her lids sewn together nor having her left eye shut with weights. I asked her if she would mind me writing to her consultant, Mr Smith, as I thought that there was something a little less dramatic that might help. She agreed, and would follow this up with Mr Smith as her routine six-monthly appointment was next month.
Unfortunately, it was a resounding No. Mr Smith felt that the cornea was so damaged and vulnerable that he didn’t want to risk anything on that eye at all.
At her next appointment with him, Mr Smith said he’d done some research about my suggestion and was happy to go along with the idea. It also helped that, apparently, I had a reasonably good reputation in ophthalmology.
Linda made an appointment for a scleral contact lens fitting. We would be using a semi-scleral or mini-scleral lens for simplicity (it’s all semantics really, if it lands on the sclera, it’s a scleral lens, right?). The fitting went well and the lens was made.
“When Keith applied the first lens, I cried. I could see the leaves on the trees opposite-clearly!” Linda wrote.
“My life is full again and I’ve taken up my old activities. My vision is clear and bright, and I no longer dread the winter and its long hours of dim light.
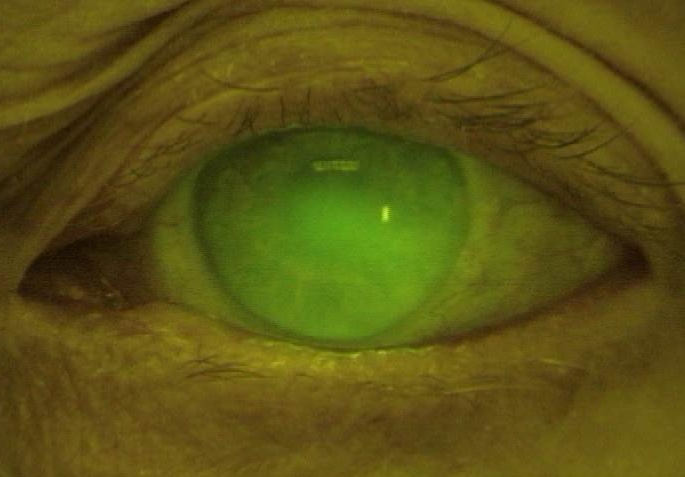
Scleral lens fit with fluorescein in tear reservoir
“I was offered hope, when there was none. Keith never gave up – and consequently, he gave me back the priceless gift of sight.
“I hadn’t realised just how much the loss of it impinged upon my whole life, influencing many parts of it. I am now 85 and doing anything I like, driving, accepting invitations and enjoying every day. In fact, I can see better than I ever have done.
“I will never stop being thankful to him for persevering when others had given up.”
Trusting in teamwork
Now don’t get me wrong. This was not a case of ‘one lens fit and everything is perfect’. There were several adjustments initially and, over the years, I have tried to improve the fit each time we make a new lens.
The scleral lens is doing two things. Firstly, it is helping to improve and maintain the corneal health and minimise the dry eye symptoms, to the point that the drops are instilled into the lens bowl on application and no more are needed during the day.
Secondly, the way that the lens holds liquid over the irregular corneal surface eradicates the distortion and, hence, improves Linda’s vision.
The current lens is yielding amazing results in comfort, vision (LE now 6/7.5) and corneal rehabilitation,
Full credit is due to Mr Smith, for having an open mind to research and explore new ideas and to have trust in those implementing it. He sees us as Linda’s team; he looks after her dry eye symptoms and oversees the corneal wellbeing that the scleral lenses have dramatically improved over the years. He has told her what the lenses have done is nothing short of miraculous. But that’s scleral lenses for you, tiny little plastic miracles.
As a profession, we have the amazing ability and opportunity to restore sight and change lives beyond measure. It is a mighty, yet humbling thing.
If you don’t fit scleral contact lenses yet, do investigate it. It’s not as scary as you think.
Keith Tempany FBDO CL FBCLA qualified in 1976 and worked in both independent and multiple practice before opening a fee-based contact lens only practice in 2002. He is a fellow and a past president of the British Contact Lens Association (BCLA) and oversaw the development and launch of its Myopia Management Certificate. Keith is the store director of Leightons & Tempany Opticians & Hearing Care in Poole, and works as an independent consultant. He is an experienced author, lecturer and facilitator of contact lens and dry eye education both nationally and internationally.
Cover image from stock.