Our phone lines are currently down, we apologise for the inconvenience

Focus on … DED pathophysiology
Pathophysiology of dry eye disease
Pathophysiology3 is the disordered physiological processes associated with disease or injury.
The core mechanism of DED is tear hyperosmolarity induced by evaporation. which causes damage to the ocular surface by initiating a cascade of inflammatory events which in turn become what has been termed the vicious circle of DED.(Fig 2)
If we consider the two principal forms of DED, ADDE and EDE, the process is slightly different.
In ADDE tear hyperosmolarity is induced by a reduction in lacrimal production in an otherwise normal evaporative condition.
In EDE the hyperosmolarity is caused by excessive evaporation where the lacrimal gland is functioning normally.
Since hyperosmolarity is at the core of evaporation in both forms, all forms of DED are in a sense evaporative, so we should consider EDE to be more of a hyper-evaporative state.
The tear hyperosmolarity is in essence the trigger for the cascade in DED initiating signalling events in epithelial cells leading to inflammatory mediators and proteases being released, this in turn causes goblet and epithelial cell damage and loss and damage to the glycocalyx.
The result is the characteristic punctate epitheliopathy, tear film instability and reduced tear break up time (TBUT). This reduction in TBUT completes the vicious circle by amplifying the hyperosmolarity and so the perpetuation of the disease.
There are potential outside factors which may influence a shortened TBUT such as ocular allergic reactions, contact lens wear and reactions to topical preservatives, which would then be considered to be the primary cause for the tear hyperosmolarity.
Causes of ADDE are varied. Topical anaesthesia or sensory interruptions to the lacrimal gland can cause reduced lacrimation or blink rate, also trigeminal nerve damage or refractive surgery. Obstruction to the lacrimal ducts may result from cicatricial conjunctival disease. Certain drugs in systemic use, such as antihistamines, beta-blockers, antispasmodics, diuretics and some psychotropic drugs are also a risk factor for DED. Most common in the western world is the association with auto immune diseases such as Sjogren’s syndrome.
EDE results from the loss or reduction of an evaporative barrier function of the tears or as a result of reduced surface wettability. The most common cause is from Meibomian Gland Dysfunction (MGD) This is a topic in its own right and some of the mechanics of MGD are still not fully understood. As a summary gland hyperkeratinisation, blockage and drop out will affect supply of meibum to the tear film which reduces the lipid layer leading to a reduced TBUT and tear film instability and evaporation. Meibum quality, oil composition and increased viscosity is another factor which can affect expressability, exacerbate obstruction of the gland openings and therefore lipid deficiency.
Fig 2: The pathophysiology of DED3
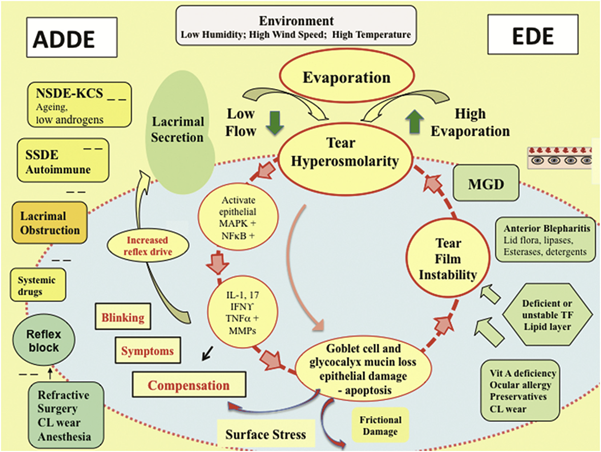
Adapted from Bron A.J. (2015) The Definition and Classification of Dry Eye Disease. In: Chan C. (eds) Dry Eye. Essentials in Ophthalmology. Springer, Berlin, Heidelberg. https://doi.org/10.1007/978-3-662-44106-0_1
Read more about dry eye disease
- Introduction, role of the dispensing optician
- Definition and classification of dry eye disease
- Pathophysiology
- Prevalence and epidemiology
- Diagnosis
- Assessment
- Management
- Education
- References and further reading