Dry Eye Corner Part 3
TFOS DEWS III delivers all the science in one place (courtesy TFOS DEWS III report)
There are many different ways and levels to start and dry eye clinic, just as there are many different work and financial resources and settings. In this article, I will share my own experiences and thoughts, and hopefully, inspire some of you to take that next step.
Knowledge is key
Firstly, knowledge is key. Running a dry eye clinic requires a certain skill set and knowledge base, and there are many ways to attain this – including attending lectures, CPD events, and even getting help from those who have already setup a dry eye clinic.
ABDO regularly offers professional development opportunities around dry eye disease and management through Dispensing Optics journal as well as in-person and online CPD sessions, which are promoted online in its Events section. The Association also has a Focus on Dry Eye Disease (DED) section within its Clinical Hub.
Other online courses, such as the British Contact Lens Association Dry Eye Management and Contact Lens Retention Certificate, can validate your claim to be a ‘dry eye expert’ and give you an independently-judged certificate to hang on your wall to prove it.
I’ve always believed that carrying out evidence-based practice is important; this isn’t merely about backing up opinions with data; it’s a systematic, structured approach to decision-making that focuses on finding the best available scientific evidence – and integrating this with your individual clinical experience, along with the patient’s own values and choices.
Providing the evidence
I have found that using scientific evidence to validate your recommendations reassures patients, and creates the solid foundations for a good patient-practitioner relationship – because most of your dry eye patients will be with you for a long while.
Crucial to this evidence-based practice, in the author’s opinion, is the recently-published Tear Film and Ocular Surface Society Dry Eye Workshop (TFOS DEWS) III1, which looks at all the science for you and delivers it in one place, making it the gold standard in dry eye guidance.
TFOS DEWS III even gives you algorithms to diagnose DED2 – along with algorithms for management and therapy regimes3 – something which was not available 26 years ago when I started my clinic.

L-R: Fluorescein corneal staining illuminated with a blue light; lissamine green bulbar conjunctival staining under white light; lissamine green staining of lower lid wiper epitheliopathy under white light (courtesy TFOS DEWS III report)
Investing in the right equipment
Some practitioners may have concerns about investing in the latest equipment and this undoubtedly discourages many eyecare practitioners from opening a dry eye clinic.
But setting up a dry eye clinic doesn’t necessarily require a heavy investment initially; you most likely already have the basics, i.e. a slit lamp and fluorescein, add in lissamine green and you have all the basics required to diagnose DED according to the TFOS DEWS III Diagnostic Methodology Report2.
The modern diagnostic tests and treatments out there are excellent, but you don’t need all of them to begin or run a successful clinic. I would, however, strongly suggest that a good imaging system on your slit lamp is an excellent educational tool for showing your patients the extent of their problem and for monitoring their progress through various treatments. For many patients, this is literally an eye-opener.
Time is money
It is often said that ‘time is money’ and I couldn’t agree more. Allowing enough time to go through history and symptoms, carry out a full dry eye examination, show the patient all the test results and images and discuss treatment recommendations, is fundamental to how much you will charge for this appointment.
I have found that one of the most frequent comments new patients make is how supportive it is to have someone take the time to listen, but also to explain the nature of their problem for a change.
How much you charge for this is up to you; I merely calculated how much clinic time I had available and how much the total practice outgoings were to calculate how much per minute I should be charging. Patients will generally value the quality of that time you take with them.

A potential pitfall is missing asymptomatic patients during a routine slit lamp examination
Common pitfalls to avoid
As with any business model, over-investing too early (when you don’t need to) can create unnecessary difficulties and pressure, and setting up a dry eye clinic is no different.
Build on the basics and reinvest when you can in more advanced diagnostics, perhaps testing for tear osmolarity or MMP-9 inflammatory markers; maybe then look at combined tear film analysers, which can carry out meibography and objective tear film measurements later, when you are more established.
Another potential pitfall is missing asymptomatic patients during a routine slit lamp examination, be it during an eye examination or contact lens aftercare appointment. Many patients will have some degree of meibomian gland dysfunction prior to symptoms appearing. If these symptoms are ignored, it could lead to contact lens dropout or to more serious symptomatic DED.
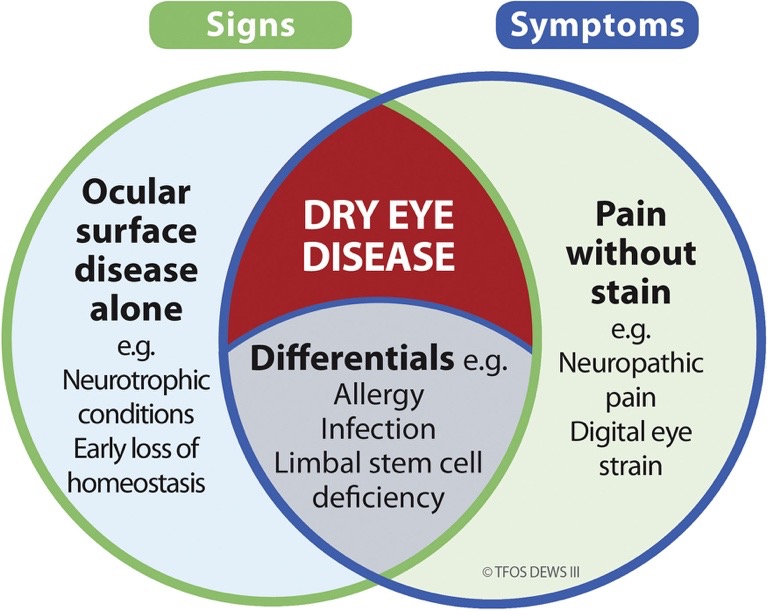
Although DED is classified as having both signs (of loss of homeostasis of the tear film and/or the ocular surface) and symptoms, ocular surface signs in the absence of symptoms reflect the presence of ocular surface disease, but do not signify the existence of DED specifically.
Follow-up appointments are essential because DED is a chronic, progressive condition and, as such, requires ongoing management. There is no one-time cure. These appointments will allow you to monitor the effectiveness of the treatment, to adjust therapies if necessary, prevent long-term corneal damage and ensure the patient’s well-being and persistence with their current regimen.
These appointments also enable you to manage the chronic nature of the disease. Failure to encourage these appointments can be catastrophic to your dry eye business.
References
1. Perez VL, Chen W, Craig JP, Murat Dogru, Jones L, Stapleton F, Wolffsohn JS, David A. Sullivan DA. TFOS DEWS III. American Journal of Ophthalmology 2025 Sep 23:S0002-9394(25)00516-1. doi: 10.1016/j.ajo.2025.09.038.
2. Wolffsohn JS, Benítez-del-Castillo JM, Loya-Garcia D et al. TFOS DEWS III: Diagnostic Methodology. American Journal of Ophthalmology 2025 Nov:279:387-450. doi: 10.1016/j.ajo.2025.05.033.
3. Jones L, Craig JP, Markoulli M et al. TFOS DEWS III Management and Therapy Report. American Journal of Ophthalmology 2025 Nov:279:289-386. doi: 10.1016/j.ajo.2025.05.039.
Next month, Keith will explore the role of dispensing opticians, optical assistants and receptionists in identifying those patients who might be suffering from dry eye.
Keith Tempany FBDO CL FBCLA qualified in 1976 and worked in both independent and multiple practice before opening a fee-based contact lens only practice in 2002. He is a fellow and a past president of the British Contact Lens Association (BCLA) and oversaw the development and launch of its Myopia Management Certificate. Keith is the store director of Leightons & Tempany Opticians & Hearing Care in Poole, and works as an independent consultant. He is an experienced author, lecturer and facilitator of contact lens and dry eye education both nationally and internationally.